Pectus Excavatum
The Chest Wall Deformity program at Johns Hopkins All Children’s Hospital evaluates and treats children and young adults with pectus excavatum.
The Johns Hopkins All Children’s Chest Wall Deformity program consists of highly qualified surgeons committed to improving the lives of patients with pectus excavatum. Our surgeons are specially trained to diagnose and treat pectus excavatum and have extensive experience using the Nuss procedure, a minimally invasive way to repair the condition. We use the latest surgical and care techniques and work closely with specialists across our hospital to provide patients and families with the highest quality of care. In addition to patient care, our team is leading regional and national discussions on pectus excavatum diagnosis and repair and through research, has developed new methods to determine the severity of chest wall deformities.
 Picture of a severe pectus excavatum.
Picture of a severe pectus excavatum.What is Pectus Excavatum?
Pectus excavatum is the most common chest wall deformity, occurring in about one in 500 children and accounting for more than 90 percent of congenital chest wall deformities. Pectus excavatum is where the sternum and ribs develop abnormally, causing the sternum to drop inward toward the spine and produce a caved in or sunken appearance of the chest. This condition progresses throughout childhood and is sometimes referred to as “funnel” chest. Pectus excavatum is usually diagnosed within the first year of life and is three times more common in boys than girls.
Causes
The exact cause of pectus excavatum is unknown. Recent information suggests causes may be linked to:
- A genetic component
- An imbalanced growth of the sternum and ribs
- Musculoskeletal disorders such as scoliosis and Marfan syndrome, which suggests abnormal connective tissue (note: the majority of patients with pectus excavatum do not have musculoskeletal disorders)
Symptoms
Often, patients don’t have any symptoms. Some patients, however, may experience:
- Chest pains
- Shortness of breath
- Difficulty exercising
- Psychological symptoms, such anxiety or poor self-esteem
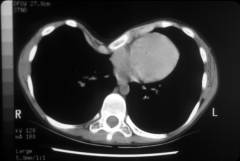 CT scan showing the sunken in breastbone.
CT scan showing the sunken in breastbone.Pectus Excavatum Evaluation
Each patient diagnosed with pectus excavatum undergoes a thorough history and physical examination. Our team is developing new ways to measure and assess chest wall deformities. Some children, however, may still need computed tomography (CT) scans or magnetic resonance imaging (MRIs) prior to their procedure. A comprehensive pre-operative evaluation often includes cardiac and pulmonary testing.
Pectus Excavatum Repair
There are several surgical options to correct pectus excavatum. Our experts most often use the Nuss procedure, which is a minimally invasive approach to repair pectus excavatum.
 Picture of a Lorenz bar.
Picture of a Lorenz bar.About the Nuss Procedure
The Nuss procedure involves two small incisions made on each side of the chest. A second small incision is made on the right side of the chest to allow for a scope (small camera) in order for the surgery team to watch the procedure inside the chest. A metal bar spanning the width of the chest is implanted under the sternum in the chest cavity. The bar lifts up the breastbone and corrects the deformity over time. Typically, the bar is left in place for two to three years.
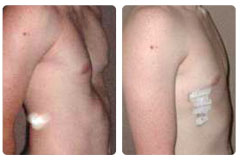 Picture of a patient before and after repair of the pectus excavatum.
Picture of a patient before and after repair of the pectus excavatum.Nuss Procedure Recovery
Our team has developed a recovery plan focused on patient comfort, a quick return to activity and an avoidance of urinary catheters, epidural catheters and excessive testing while hospitalized. This recovery pathway has been so successful that the results have been published in scientific medical journals. Also, part of our recovery plan is breathing exercises and walking. Most patients spend two days in the hospital and are able to resume their full activities, including sports and weight lifting, by three months. Some contact sports might be restricted longer, such football and hockey and sports that require swinging like golf.
Pain Management
Our team uses patient-controlled anesthesia and works very closely with our pain management team to help control postoperative pain.
Our team also has developed an enhanced recovery pathway plan that focuses on patient comfort, a quick return to activity and an avoidance of urinary catheters, epidural catheters and excessive blood and X-ray testing while hospitalized.
Research
The Department of Surgery at Johns Hopkins All Children’s Hospital is active in pectus excavatum research. Our team has led regional and national discussions on pectus excavatum diagnosis and repair, and is researching several topics, including the practice variation of pectus excavatum repair to new methods for determining the severity of chest wall defects.
Contact Us
Questions?
We know you want what's best for your child. We're ready to assist you with your questions. Call 727-767-4170.

Request an Appointment
Complete our online form and our team will reach out to you shortly to schedule an appointment.
Call toll-free 800-456-4543 , ext. 4170.